The NMHS 2 is proposed with the following objectives:
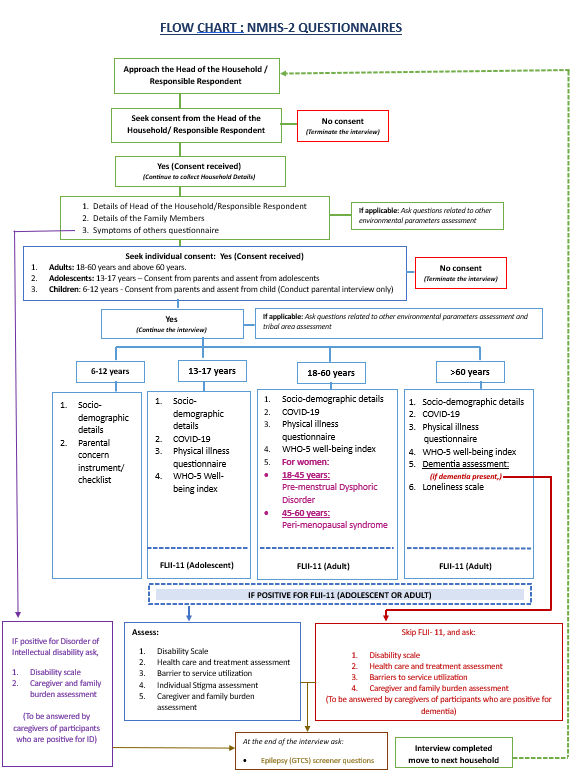
The National Mental Health Survey 2 (NMHS-2) is a large-scale, multi-centre national study to assess the prevalence, patterns, and characteristics of mental health problems among individuals aged 18 years and above (adults) and adolescents aged 13–17 years across all States and Union Territories of India.
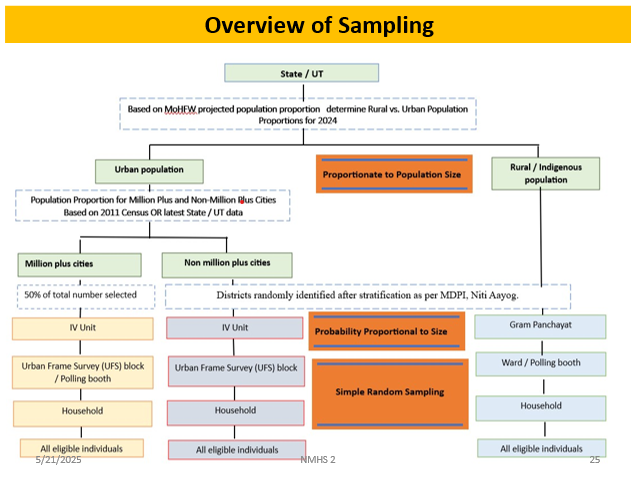
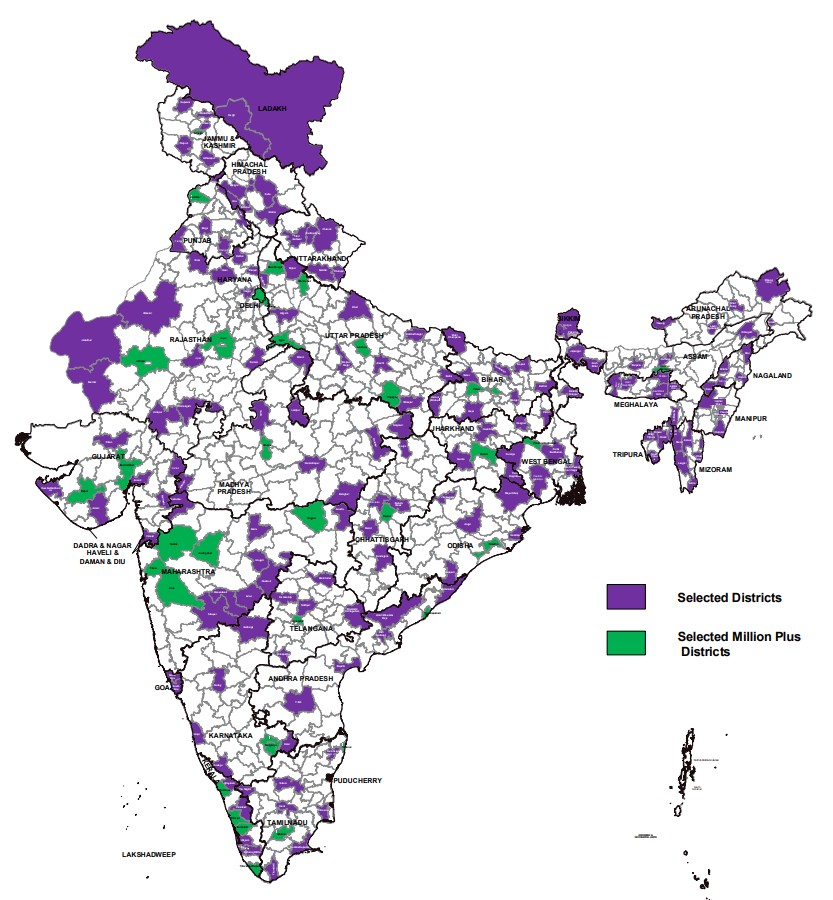
A multi-stage, stratified, random cluster sampling method with population proportionate to size (MSRS-PPS) is used to ensure state-level representation.
As part of NMHS-2, informed consent is obtained from each participant before data collection, ensuring voluntary participation. Participants are informed about the purpose of the survey, confidentiality of their responses, and their right to withdraw at any time. Consent is documented in accordance with ethical guidelines and protocols.
The details of the individual members collected from the head of household would automatically get filled into the socio-demographic form. Record details about education, occupation, and Income (BPL/APL).
A 3-item Loneliness Scale is to be asked to all individuals above 60 years of age for assessment of subjective perception of social isolation in the elderly.
A disability scale was considered necessary for the NMHS-2 as the Sheehan’s disability scale used in NMHS-1 had become paid.
These questions are to be asked only if the respondent is positive for any of the FLII-11 disorders.
These questions are to be asked only if the respondent is positive for any of the FLII-11 disorders and are to be asked to the primary caregiver.
Screening questions for PMDD includes assessment of physical and mental symptoms causing dysfunction associated with pre-menstrual period in women of ages 18-44 years.
This checklist assesses the concerns of parents about their children (aged 6-12 years) on various domains related to mental health and neurodevelopment.
Assesses the capacity and quality of care facilities.
This section contains screening questions about symptoms of mental illness in the members of the family and is to be answered by the head of the household.
This section addresses the need to understand the overall wellbeing of the individual with respect to their mental health.
The FLII-11 which is the compatible to the ICD-11 is the primary assessment instrument for the NMHS-2 to assess psychiatric morbidity.
These questions are to be asked only if the respondent is positive for any of the FLII-11 disorders.
Gauges personal experiences and perceptions of stigma.
Epilepsy manifests in various forms, with Generalized Tonic Clonic Seizures (GTCS) being the most prevalent, accounting for approximately two-thirds of cases and easily recognizable.
These questions will be asked to all individuals above 60 years of age and everyone above 45 years of age who has screened positive in ‘Symptoms of Others’ for possible neurocognitive disorder.
Evaluates state-level mental health infrastructure.
To ensure consistency and quality in data collection, NMHS-2 will implement multiple types of ongoing training:
A centralized Training of Trainers (ToT) program is being conducted by the NIMHANS team for State and UT coordination teams. These trained teams are then conducting training for local field teams, covering didactic sessions, clinical observations, case discussions, and digital data collection techniques. A detailed survey manual is guiding the training process. By April 30th, 2025, 24 states have completed the 6-week training program, and 3 states are undergoing training.
Conducted monthly online by a central team psychiatrist, this training reinforces key concepts, addresses field challenges, and ensures standardized survey administration.
A three-hour online session designed for resource persons to support survey teams in resolving technical and methodological queries during implementation.
Monthly in-house training sessions are conducted for NMHS-2 Survey Coordinators and Field Data Collectors to supplement state and refresher training. The sessions cover key components like sampling methodology, FLII, and additional questionnaires to strengthen field practices and ensure readiness.
To maintain high standards of quality assurance in NMHS-2, several steps are integrated into the study protocol:
Mental Health Dialogue is a platform, to facilitate academic interaction and for enlisting likeminded people, who have committed for the conduct of NMHS 2. This interaction is meant to help public mental health become a bigger part of public conversations and planning.

Adopting the standard methodology, NMHS 2 would provide
Prevalence estimates of any mental health problem in the surveyed states
Pooled estimates at the national level (as per ICD / DSM)
Pooled estimates on the Prevalence of psychoses at the national level
Prevalence estimates at the state and national level of
Anxiety disorders, mood disorders, substance use disorders (Alcohol and Tobacco dependence), Somatoform disorders, Illness anxiety disorders, Internet and Gaming disorders including technology addiction
Screener positives for Epilepsy (GTCS only), Behavioural and Cognitive problems
Characterise Burden of illness on the family, Health care seeking pattern and service utilization among those with any mental health problem / epilepsy
Current level of services and resources for mental health care in the surveyed states
Recommendations to improve mental health services
Availability of data on select determinants of mental health (reported physical ailments, migration, climate change, Tribal areas, etc.,) which will help examine macro and micro issues
The expected outcome of MHSA and Resource mapping are
Status & implementation of MHCA, 2017 at State / UT
MHHR: Mental Health Professionals; Health Professionals trained in Mental Health; Health Staff trained
Inventory of Mental Health IEC
Documenting best practices in Mental Health Service delivery
Estimating treatment and coverage in Public and private health care institutions for mental health and documenting mental illness morbidity pattern
Listing State / UTs wise challenges for enhancing service delivery